This three-part series on Data Science as Resistance was originally developed through a collaboration between Cat Fraser of Co-EQ and the Data Science for Health Equity network. While Co-EQ continues to incubate the design of the technology supporting this work, Lab of Lived Experience (Lab OLE) is our community partnership to accelerate health equity, change and innovation.
We are sharing this content here to highlight our approach to community-led pandemic decision making.
We invite you to join us.
Part 1: My Journey - The Frontline of the Ongoing Pandemic
On the 5th anniversary of International Long COVID Awareness Day, buildings worldwide were lit up in teal, grey and black, united behind one clear message: we demand a cure. This powerful visual demonstration was followed by UK-wide protests asking #WhereIsIt—referencing not just the £100M annual funding requested by the Coronavirus All-Party Parliamentary Group in 2022 that remains unfulfilled, but also demanding dedicated research centres, specialised treatment protocols, and workplace accommodation policies that acknowledge the fluctuating and severity of our energy-limited conditions.
“The APPG recommends that the £50m pledged for long COVID research is doubled to £100m and matched each year to support the development of new treatments for long COVID. There is an argument that the NHS needs to take a more urgent, imaginative approach” - UK Coronavirus APPG 20221
These public actions represent a new form of real-world data visualisation, making visible the catastrophic impact on hundreds of millions worldwide who cannot recover or return to normal life. They honor those whose suffering often remains invisible to society and healthcare systems and those who are dying without recognition or support.
My journey2 with these invisible illnesses began years before the pandemic. After contracting severe Glandular Fever at university, I was diagnosed with ME and experienced a severe attack in 2009. This personal adversity unknowingly prepared me for what was to come. When COVID hit me in early 2020, I found myself once again navigating a medical system fundamentally unprepared for complex chronic illnesses—only this time, millions were joining me.
The parallels between ME and Long COVID reveal a critical truth: our healthcare frameworks were never designed to address multi-system, multi-organ diseases that exist outside traditional, siloed medical models.
Today, as hundreds of millions face similar challenges, we have both a growing public health crisis and an unprecedented opportunity to transform how we understand, treat, and support those with complex chronic conditions.
Quantifying the Invisible Struggle to Find Healthcare
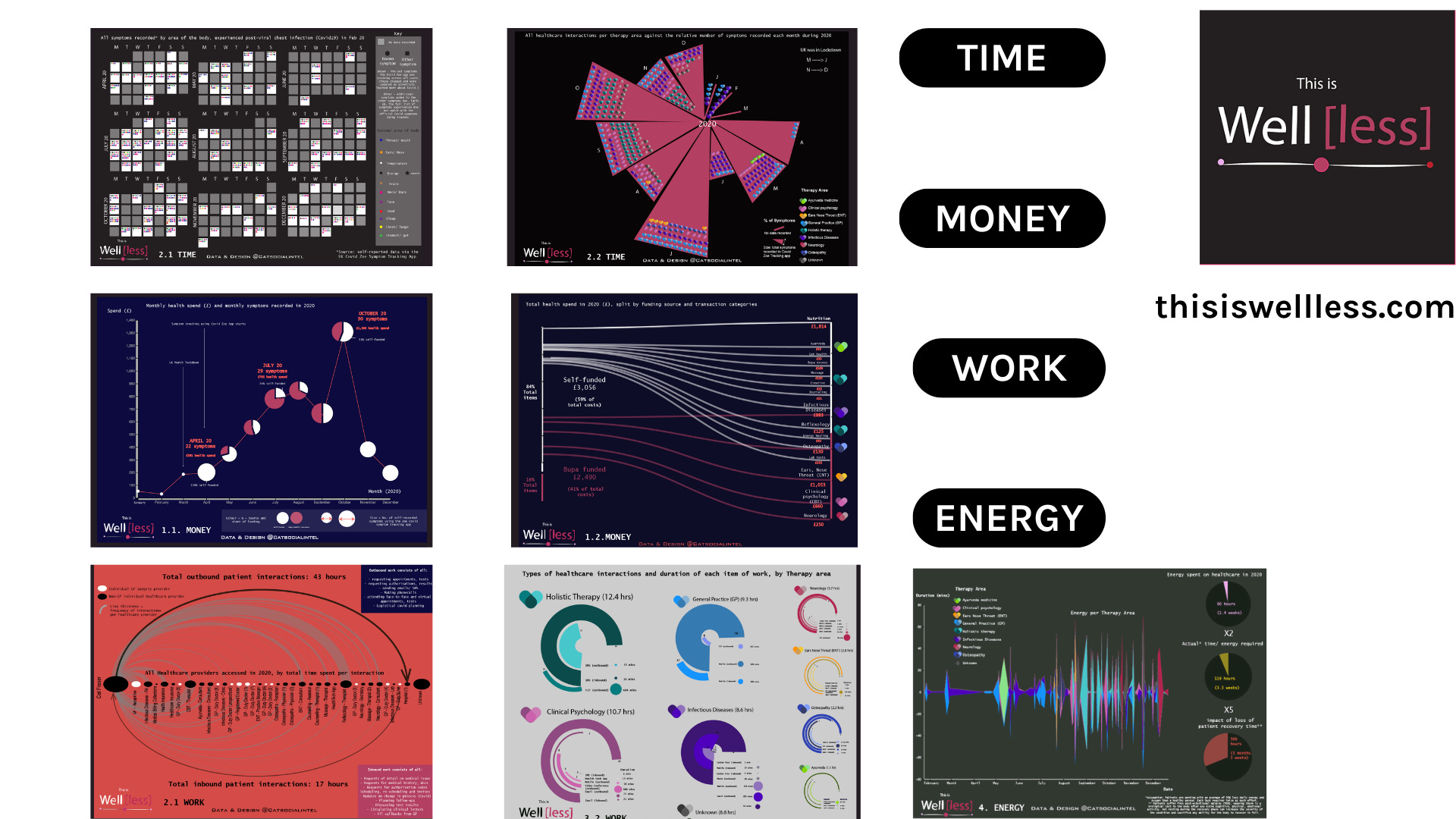
In 2021, I created a self-data project to bring to life my (mostly private) health customer journey through a siloed-system - analysing and visualising the costs through four chapters: time, money, work and energy.
A quarter of my working life lost in 2020 trying to find healthcare that didn’t exist
Since then, I have watched institutions fiercely defend their business as usual practice and politicians design a future of health that doesn't factor in any of the changes our communities need right now.
The Ongoing Pandemic Reality
Despite widespread messaging to the contrary, the COVID-19 pandemic remains an active, evolving threat:
Latest data from Wales4 shows nearly 80% of hospital recorded COVID cases were from hospital-acquired infections, highlighting ongoing airborne transmission in healthcare settings
At least 11,0005 people died in the UK from preventable airborne COVID infections in 2024 alone
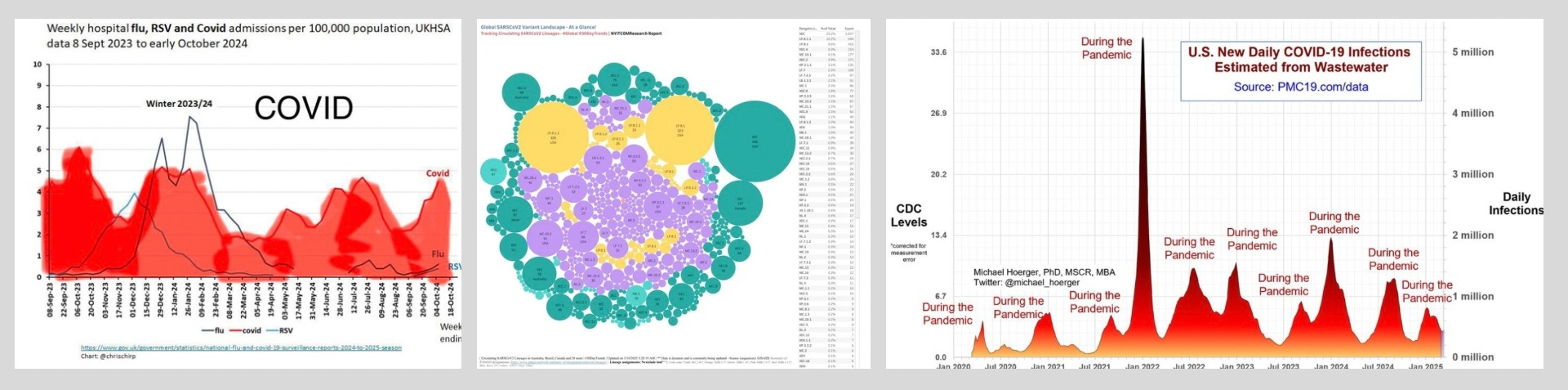
New variants continue to emerge and circulate widely, as evidenced by the complex "variant soup" landscape6 (see below)
Last year, the UK had both large winter and summer waves and despite some respite from covid this winter, we are still in a 'quademic'7 along with a troubling rise of TB, Measles and other diseases due to weakened immune systems from repeated inhaling of airborne particles89
America peaked at 10K infections per day in January and 1K deaths per week10
Despite countries dismantling most data reporting and surveillance (which the WHO continues to warn against), here are three data sources that the Covid-Aware have been following closely to stay informed:
This isn't a post-pandemic era—it's a pandemic being systematically ignored despite overwhelming evidence of its continued impact and extensible threat to public health.
Every Covid infection is causing climate change to the human body
Just as climate change creates cumulative, often irreversible damage to our environment, repeated COVID infections cause progressive damage to multiple body systems and organs. Each "mild" infection may lead to microvascular injury11 neurological changes12, and immune dysregulation that compounds over time13 making recovery increasingly difficult.
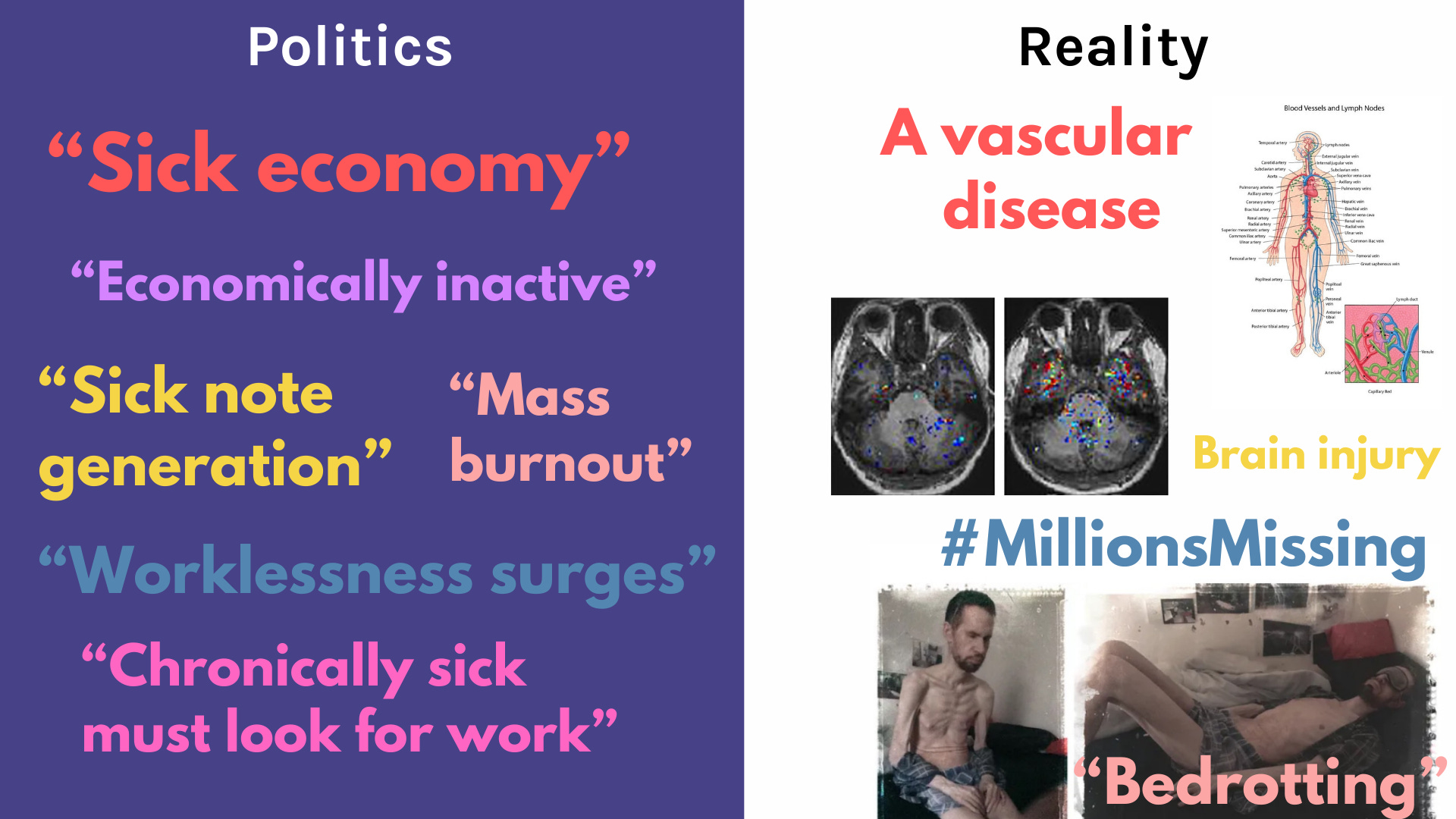
The disconnect between political framing and biological reality couldn't be starker. While politicians talk about "sick notes," "economic inactivity," and "worklessness” surges, the medical reality reveals:
A vascular disease, often affecting the entire body
Significant brain injury from each ‘mild’ infection
Multi-system, multi-organ dysfunction causing people to fall out of work and society 14
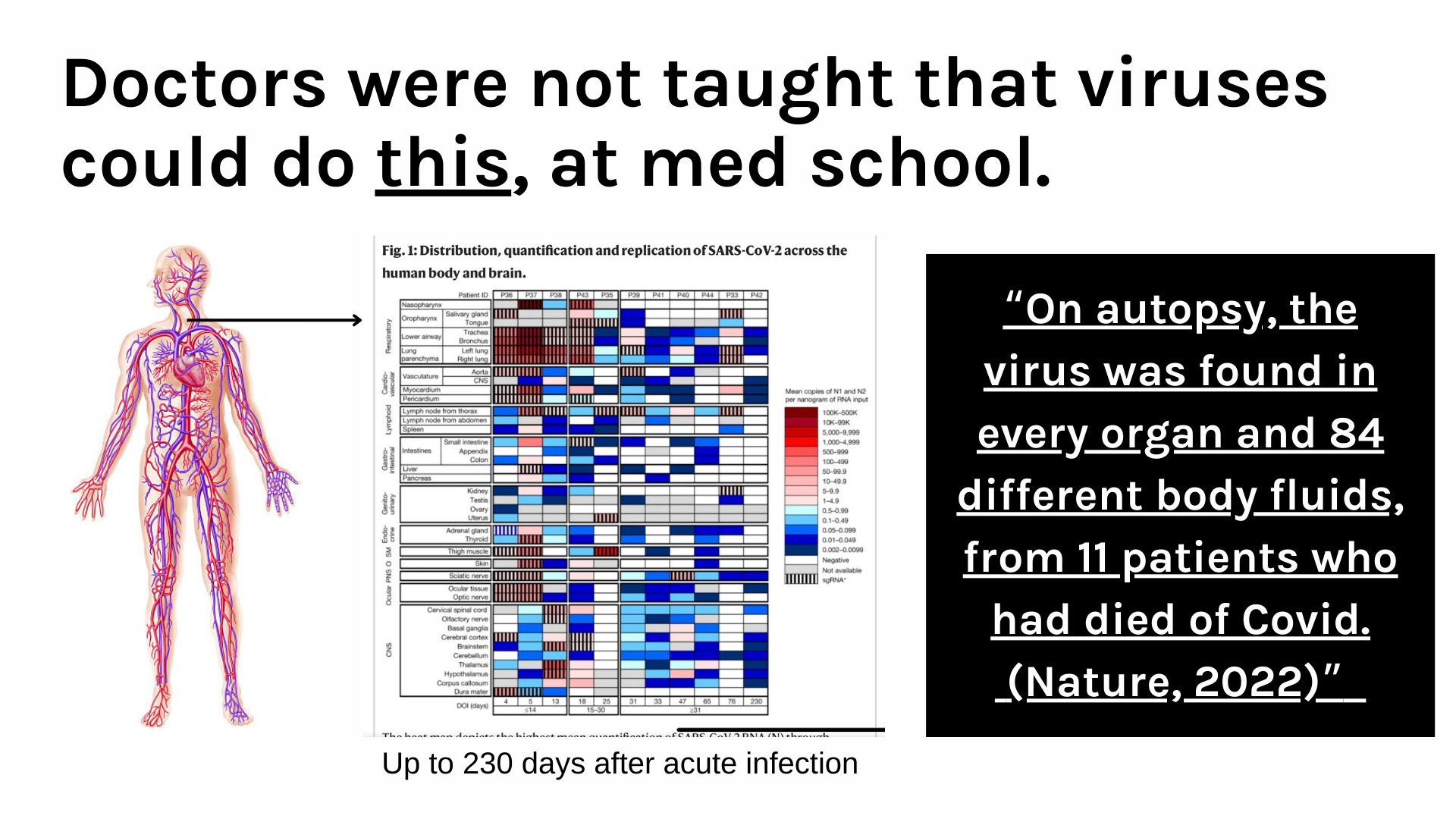
SARSCOV2 the virus, persists in the body up to 230 days after acute infection, a fact that most healthcare providers weren't taught in medical school.
"On autopsy, the virus was found in every organ and 84 different body fluids, from 11 patients who had died of Covid." (Nature, 2022)15
The Workforce and Economic Crisis is Just the Tip of the Iceberg
The UK is experiencing its largest surge in economic inactivity in decades, with over 2.8 million16 people now classified as "long-term sick" and unable to work. When compared to pre-pandemic trends, this represents an excess of approximately 850,00017 people who have fallen out of the workforce—a figure that closely tracks with conservative estimates of those with debilitating, daily Long COVID18.
What makes this inevitable workforce crisis particularly devastating is that:
The UK government claims it is "supporting people" by pushing them back to work, yet medically, millions are physically unable to work
Benefit reductions and even harsher work capability assessments are creating poverty, not recovery
Many affected are in their prime career years (30-50), with limited safety nets
Current policies are treating a biomedical crisis as if it were a motivational one
And this is only the tip of the iceberg.
The harsh reality is that an estimated 400 million+19 people worldwide are struggling with Long COVID, ME/CFS, and other infection-triggered conditions that the medical system cannot yet adequately treat, and so many more will continue to end up here. No amount of "back to work" incentives can overcome neurological damage, vascular disease, and multi-system dysfunction.
In Part 2, I'll explore the complex mechanisms behind these conditions, what standard medical tests are missing, and why current approaches are mathematically unsustainable.
Subscribe to the Lab of Lived Experience Substack for updates: